

VIENNA, Austria (Reuters) — A new medical imaging technique, called Electrical Impedance Tomography (EIT), where electrodes are used to apply high-frequency currents through the body, could help doctors to continuously monitor the function of patients’ lungs during artificial respiration.
Artificial ventilation is often vital to a patient’s rehabilitation, but doctors can find it difficult to gauge the correct air pressure for every individual, with too much possibly causing lung trauma.
“Mechanical ventilation on one hand is life-saving, but on the other hand mechanical ventilation is unphysiologic and can lead to secondary lung damage, so-called ventilator induced lung damage,” said Dr Stefan Böhme from the Medical University Of Vienna.
But a new method that combines CT scans (computed tomography) with EIT data could help doctors get a better look inside the lungs of patients and identify the regional distribution of ventilation.
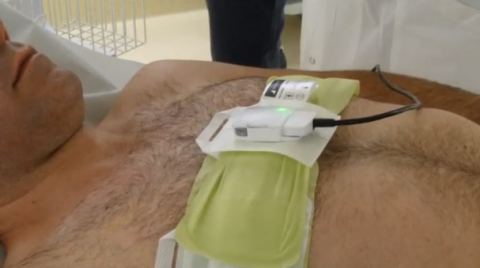
Following a standard CT scan, patients put on a chest belt with electrodes applied directly to the skin. The electrodes apply a high-frequency current through the body, though the current itself is so weak it can’t be felt. The resulting electrical voltage is measured and fed into a computer algorithm that turns it into a living – ‘breathing’ – image of the patient’s lung.
The project is a collaboration between Vienna University of Technology (TU Wien), the Medical University of Vienna and the University of Veterinary Medicine Vienna.
CT scans are high-powered X-rays that provide clear images but expose patients to between ten and 100 times more radiation than a normal head or chest X-ray, for example.
Florian Thürk, a researcher at TU Wien, said just one CT scan is needed to map a patient’s body, minimising their exposure to radiation.
“For instance, we take the contours of the thorax and we take the contours of the lungs so we know exactly where the positions of the organs are. We feed this into the reconstruction algorithms of the EIT, and with this we reduce the error and we can enhance the images and therefore the clinical parameters that result from the images,” said Thürk.
After further validation, the method would let doctors continuously monitor how their patient’s lungs are responding to mechanical respiration, and adjust the airflow as needed.
“We measure regional distribution of ventilation, so we get a bedside image showing us directly where the air of each breathing cycle goes to the lungs,” added Böhme.
The technology has so far been successfully tested on pigs, with human clinical trials now on the horizon. Thürk added that they are also working on standardising the method so that, eventually, doctors will be able to more easily calibrate artificial ventilation to an individual’s needs.
“The next step will be human clinical trials and from the data we get there we’ll try to first validate our previous results and then to contribute to EIT in a sense that it will be applicable in a clinical routine so that we get standardised parameters,” he said.
The research was published recently in the journal PLoS One.